国际肝病 发表时间:2025/5/1 23:24:24
编者按:在2025大湾区肝病国际论坛暨消除病毒性肝炎大会上,英国伦敦帝国理工学院医学院客座教授、前世界卫生组织(WHO)日内瓦总部艾滋病毒、肝炎和性传播部门资深科学家Philippa Easterbrook教授分享了肝炎治疗领域的革新性策略框架,本刊特对Easterbrook教授围绕相关话题进行专访。Easterbrook教授指出,为加速实现肝炎消除目标,需打破传统医疗模式,推行“去中心化、整合服务、任务转移”三重策略。她深入剖析了三重策略的实际内涵:去中心化旨在将检测与治疗资源下沉至基层卫生机构,使患者就近获得服务;整合服务通过将肝炎护理嵌入现有卫生平台,优化资源配置效率;任务转移则通过培训非专科医护人员,缓解专科人力资源短缺问题。
《国际肝病》
WHO指南强调了“去中心化、整合服务和任务转移” 是扩大乙型肝炎及丙型肝炎治疗可及性的关键策略。您能解释一下这些概念的实际含义吗?
Easterbrook教授:“去中心化、整合服务和任务转移”是三大关键策略,它们在扩大HIV治疗覆盖方面发挥了重要作用,如今正越来越多地应用于改善乙肝和丙肝等其他疾病的检测和治疗可及性。
所谓“去中心化”,是指将检测和治疗服务从传统的医院和专科医生体系下沉至基层卫生机构,如初级保健诊所、社区卫生中心、为注射吸毒者提供的减害中心、HIV诊所,甚至监狱卫生服务机构等。这一过程可以是“完全去中心化”(检测和治疗均在基层机构完成),也可以是“部分去中心化”(如检测在社区进行,治疗在二级或三级医院进行)。
“整合服务”则是指将乙肝和丙肝诊疗服务嵌入现有卫生平台。例如,在HIV诊所中,可将肝炎护理纳入现有的HIV服务流程;在监狱场景中,可将其融入监狱整体卫生系统。这种整合与去中心化策略相辅相成——依托既有服务网络,既能提高资源利用效率,又能让患者在熟悉的环境中获得连贯的医疗服务,进一步降低就诊门槛。
而要让上述模式有效落地,“任务转移”(或称“任务分担”)至关重要。这意味着通过培训,让非专科医生、护士、助产士,甚至非实验室人员承担传统上由专科医生负责的部分任务。与单纯的“责任转移”不同,任务分担更强调卫生人员间的协作机制,通过明确分工与技能提升,形成跨层级、跨专业的医疗团队协作模式。这种策略不仅能缓解专科医疗资源紧张的问题,更通过优化人力配置,让医疗服务体系更加公平、高效。
Hepatology Digest: The 2022 WHO guidelines on hepatitis C care and treatment and the recent 2024 WHO guidelines for prevention, care and treatment of hepatitis B both highlight the importance of adopting the principles of decentralization, integration and task-sharing to promote access to hepatitis C and B treatment. Please can you explain what is meant by these concepts in practical terms?
Prof. Philippa Easterbrook: Decentralization, integration, and task shifting are three key strategies that have played a crucial role in scaling up treatment for HIV and are now increasingly being adopted to improve access to testing and treatment for other diseases, including hepatitis B and C.
When we talk about decentralization for hepatitis B and C care, we mean expanding the delivery of testing and treatment services beyond hospitals and specialists to peripheral health sites or lower level health facilities such as primary care clinics, community health centers, harm reduction sites for people who inject drugs, HIV clinics, antenatal clinics, and prison health services. This can take the form of full decentralization, where both testing and treatment occur at the same lower-level facility, or partial decentralization, where testing may happen in the community or primary care site, but treatment is provided at a secondary or tertiary hospital clinic.
Integration refers to embedding hepatitis B and C services within existing health services. For instance, in an HIV clinic, hepatitis care can be integrated into ongoing HIV testing, prevention and treatment services; in a primary care clinic, it is part of routine chronic care services, in a prison, it may be integrated into the broader prison health system. Integration and decentralization often go hand in hand— making services more accessible and efficient.
But to make this model work, task-shifting or task-sharing of key activities and roles is essential. This means training non-specialist doctors, nurses, midwives, or even non-laboratory personnel to take on tasks traditionally performed by specialists. The term task-sharing reflects better the intended outcome of shared care, recognizing the importance of collaboration and teamwork across different health cadres, rather than simply shifting responsibilities.
《国际肝病》
为何去中心化对实现病毒性肝炎消除如此重要?
Easterbrook教授:过去十年,丙肝诊疗覆盖率有所提升:2022年全球5800万慢性丙肝感染者中,36%已确诊,20%接受治疗,较2019年的20%确诊率和13%治疗率均有提升。但乙肝诊疗进展滞后:全球2.54亿慢性乙肝感染者中,仅10%确诊,2%获得治疗。这组数据凸显了检测与治疗覆盖的巨大缺口。
要缩小这一差距,必须突破传统依赖三级医疗机构和专科医生的服务框架,从根本上简化乙肝临床指南与服务模式,将医疗照护延伸至患者生活的社区层面。例如,丙肝的“当日检测-治疗”模式(基层非专科医生即可安全给予口服短疗程治疗)已被证明可行。只有让检测和治疗服务触手可及,患者才能更便捷地获取服务,也更可能坚持完成全程治疗。
本质上,去中心化不仅是技术层面的优化,更是一种以患者为中心的服务理念。患者往往希望在家门口获得“一站式”医疗照护,这种便利性对治疗的开展和维持至关重要。
因此,若想在全球范围内扩大病毒性肝炎服务覆盖,尤其是在非洲、中国等高疾病负担地区,必须推进去中心化策略,再结合整合服务和任务转移。这种模式不仅能让患者受益,更能助力卫生系统以更高效率和效果提供医疗照护。
Hepatology Digest: Why is decentralization so important to achieving elimination of viral hepatitis?
Prof. Philippa Easterbrook: When it comes to viral hepatitis, we have seen some progress with improved access to and scale-up of hepatitis C care over the last 5 to 10 years. As of 2022, around 36% of estimated 58 million individuals with chronic hepatitis C infection have been diagnosed and 20% treated, compared with 20% and 13% of 58 million in 2019). However, for hepatitis B, progress has been limited. In 2022, still only 10% of 254 million people living with chronic hepatitis B globally had been diagnosed, and just 2% had received treatment. This highlights a significant testing and treatment gap, especially for hepatitis B.
To close this gap, we need a radical simplification of both clinical guidelines and service delivery models for hepatitis B that includes expanding care beyond tertiary care and specialist-only services, as has been achieved for hepatitis C in many countries. We must bring key elements of the hepatitis B care pathway to the community level – near to where people live, so they can more easily access services, receive support to adhere to lifelong treatment and attend for long-term follow-up.
Ultimately, decentralization isn't just a technical solution, it’s a patient-centered approach. Patients consistently express a desire for care that is closer to home, where testing and treatment are available in one place. This convenience is critical for initiating and sustaining treatment. For hepatitis C care, which involves a short course of oral treatment with minimal side effects, there are now many examples of same day “test and treat” models delivered at primary care level by non-specialist doctors.
In summary, to truly scale up viral hepatitis B services globally, particularly in high-burden countries like those in African region or China, we must decentralize, integrate, and share tasks across the health system. It’s a strategy that not only benefits patients but also helps health systems become more efficient and effective in delivering care.
《国际肝病》
各国可采取哪些措施推动去中心化和任务转移?
Easterbrook教授:首要步骤是简化医疗照护流程。过去,病毒性肝炎的管理指南较为复杂,而2014年丙肝治愈疗法(尤其是新型直接抗病毒药物,DAA)的问世成为关键转折点。此前,传统长疗程聚乙二醇干扰素治疗需长期注射,成功率低且副作用较大,DAA则凭借简化高效的特点让初级保健机构承接治疗成为可能,经过培训的护士和非专科医护人员能够安全地提供治疗服务。
乙肝的发病机制和管理虽然更为复杂,但2024 WHO最新指南已大幅简化了 “谁需要治疗” 的判断标准,不仅扩大了符合治疗条件的人群范围(超过50%,过去为8%~15%),也为去中心化策略提供了更可行的操作基础。
为了推动去中心化和任务转移,各国需要采取一系列协调措施:
(1)各国应根据本国国情调整WHO的简化指南,确保其适用性。
(2)在扩大治疗覆盖之前,必须先确定需要治疗的人群。这要求各国依据本国流行病学特征制定系统性筛查策略:丙肝筛查通常针对注射吸毒者、血液透析患者等高危人群,而乙肝因在普通人群中患病率更高,需采取更广泛的筛查手段。
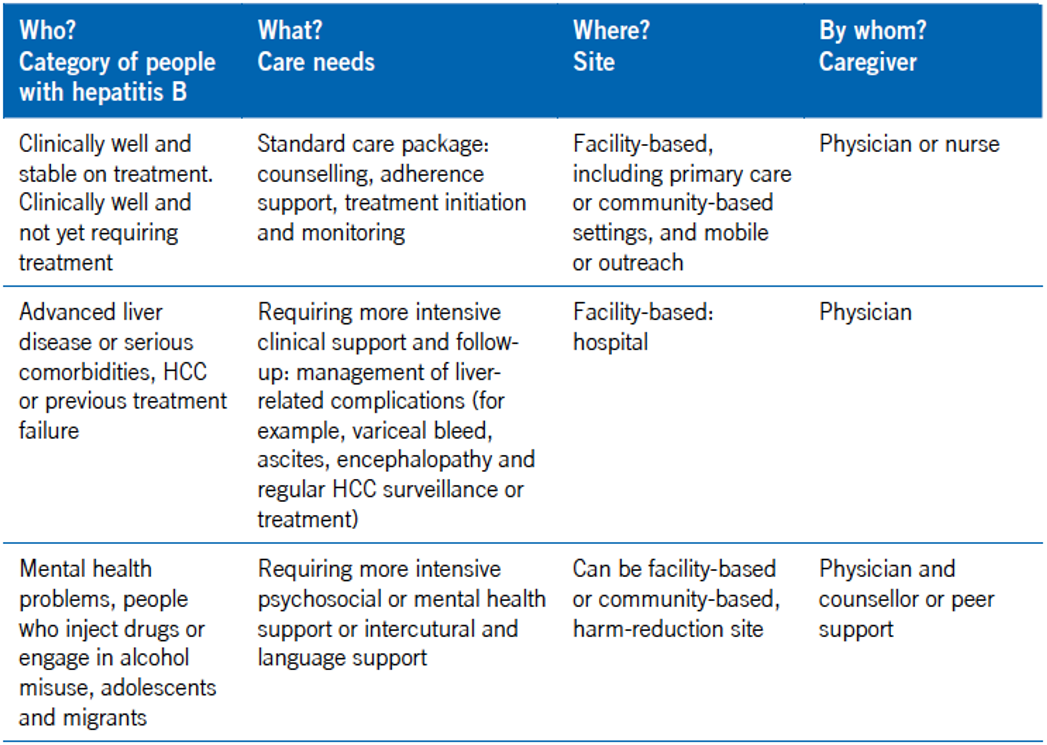
(3)建立筛查体系后,需明确服务提供框架,“差异化护理模式”在此发挥关键作用(表1)。该模式清晰界定了“谁应接受治疗”“护理在何处提供”“各级卫生机构的服务分工”及“转诊机制”,确保需要专科干预的患者及时转诊,而病情稳定的患者可在初级保健机构接受有效管理。同时,各级卫生工作者必须接受充分培训,保障操作规范与服务质量。
(4)各国需确保诊断工具和药物的持续可及性。
从简化指南、结构化筛查,到清晰的护理模式与专业培训,环环相扣的措施将助力构建高效、以患者为中心的医疗系统,为去中心化策略落地及肝炎护理可及性提升奠定基础。
表1. 潜在的差异化护理需求及慢性乙型肝炎(CHB)管理方法
(受访者提供)
Hepatology Digest: What can help countries promote decentralization and task-shifting?
Prof. Philippa Easterbrook: The first and most important step is to simplify care. In the past, guidelines for managing both viral hepatitis B and C were quite complicated. A major turning point came with the arrival of curative treatments for hepatitis C in 2014 specifically, the new direct-acting antiviral (DAA) drugs. Before these, treatment involved long courses of pegylated interferon injections with limited success and considerable side effects. The new therapies transformed the landscape. With these simplified and highly effective drugs, it became feasible to also provide treatment at the primary care level, where trained nurses and non-specialist healthcare workers could safely deliver care.
The pathogenesis and management of hepatitis B has always been more complex, but the recent 2024 WHO guidelines have made it much easier to determine who needs treatment and who does not. As a result, a significantly higher proportion of people are now eligible for treatment (more than 50% compared to 8 to 15% previously), making decentralization both more necessary and achievable.
Countries need to take a few coordinated steps to promote decentralization and task-shifting. First, through adoption of the simplified WHO guidelines and adaptation to suit their national context and healthcare infrastructure. Second, they must scale up case-finding, because treatment cannot be expanded without first identifying those with chronic hepatitis B infection and then assessing who requires treatment. This means implementing systematic screening strategies based on the country’s epidemiology. For hepatitis C, in many countries, screening can be targeted at high-risk groups, such as persons who inject drugs, or men who have sex with men. For hepatitis B, which is more widespread in the general population, a broader screening approach is needed.
Once screening is in place, countries must define how services will be delivered. The differentiated care model approach provides a helpful “Who, what, where and by whom” framework (table 1) that defines for different categories of patients – what care needs and services should be provided, where the care should take place (ie. at which level of the health system), the different care-givers who can provide these services and how to handle referrals. It ensures that patients with more advanced disease who need specialist care or other services are referred appropriately, while others can be managed effectively at the primary care level. Health-care workers must be properly trained and receive ongoing mentorship and support across these levels to ensure successful implementation.
Finally, countries must ensure consistent access to essential tools—namely diagnostics and medicines. With simplified guidelines, structured screening, clear care models, and strong training, countries can create an efficient and patient-centered system that supports decentralization and expands access to hepatitis care.
《国际肝病》
在推进过程中,目前还存在哪些缺口?您认为下一步应采取哪些行动?
Easterbrook教授:目前,许多国家仍需完成制定国家指南和操作计划以及明确如何实施肝炎检测和治疗项目这两项基础性工作,这是大规模构建有效服务体系的前提。
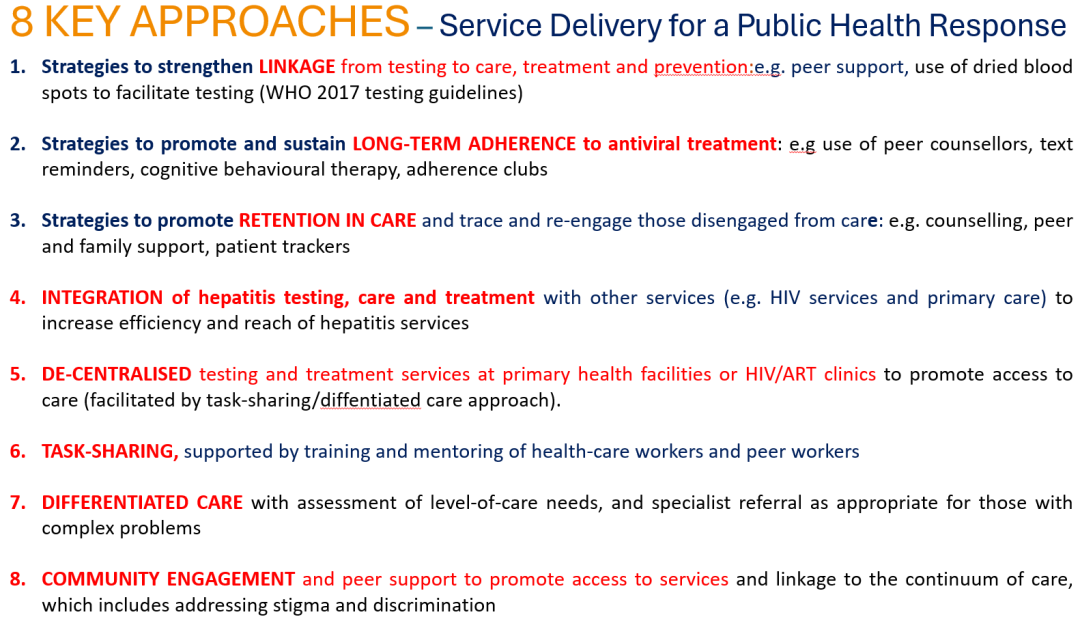
以乙肝为例,在不同地域环境和流行病学特征下,何种护理模式最具成效仍缺乏充分证据与数据支撑。这表明存在重大研究缺口,亟待通过高质量的分散式护理与共享式护理模式研究填补。此类研究需评估关键干预措施,包括促进初次诊断、建立护理联系、开展治疗评估、启动治疗方案、提供依从性支持以及确保长期护理保留等(图1)。具体干预手段可涵盖同伴支持与咨询、即时病毒载量检测、病毒载量复检策略及多月处方发放等。同时,研究需探索不同护理模式组合在不同人群和地理区域中的实际效果,这些研究成果将助力各国更高效地调整现有计划。国家相关项目在推进过程中需明确在不同环境中实施相应模式的方式。例如,城市地区以医院体系为主,而农村地区则依赖以社区检测结合初级保健的模式,让轻症患者在基层机构管理,重症患者转诊至专科医生。
此外,另一个核心挑战是保障诊断工具和治疗药物的可及性。尽管治疗可及性与成本效益已显著改善。过去十年间,肝炎治疗和普及领域取得显著成效:通过仿制药生产,丙肝药物一个疗程约60-120美元;非洲广泛使用的乙肝药物替诺福韦,年费用约30美元。然而,用于确诊丙肝活动性感染(HCV RNA 检测)和乙肝病毒载量评估(HBV DNA 检测)的分子诊断技术,其普及程度有限且成本较高,阻碍了对需治疗人群的精准指导。因此,各国仍需建立可靠的预测和采购系统以及稳定的供应链,确保诊断和药物的持续可及性。这对维持和扩大国家肝炎防控措施意义重大。
图1. 8 个关键方法——公共卫生应对的服务提供
(受访者提供)
Hepatology Digest: What are the current gaps, and what should be the next steps?
Prof. Philippa Easterbrook: Currently, one of the main gaps is that many countries still need to develop their national guidelines and operational plans outlining how they intend to implement their national hepatitis testing and treatment programs. This foundational work is critical for setting up effective service delivery at scale and involves a partnership between Ministries of Health and front-line clinicians.
National programmes then need to determine how these models should be implemented in different settings. For example, in urban areas, it may be appropriate to primarily rely on network of existing hospital-based clinics. In contrast, rural areas might benefit more from community-based testing and primary healthcare delivery, with straightforward cases managed at the primary care level and only complicated cases referred to specialists at the hospitals.
去中心化、整合以及任务转移:消除乙肝病毒感染的全球策略
世界卫生组织指南更新
(来源:《国际肝病》编辑部)
声明:本文仅供医疗卫生专业人士了解最新医药资讯参考使用,不代表本平台观点。该信息不能以任何方式取代专业的医疗指导,也不应被视为诊疗建议,如果该信息被用于资讯以外的目的,本站及作者不承担相关责任。